|
Scanning those tortuous Carotid vessels can sometimes be tricky! So here we'll go through 5 quick scanning tips to help you get great carotid images and accurate velocities.
Get Our FREE SCANNING TIP DOWNLOAD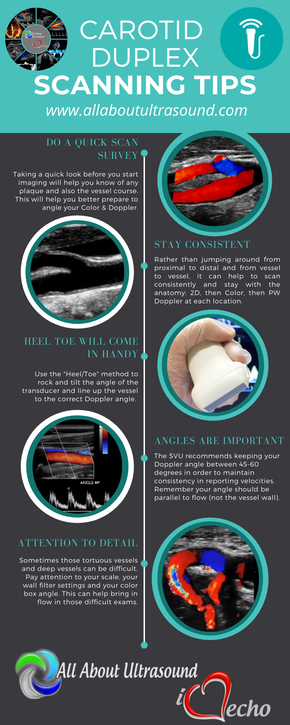
1 Comment
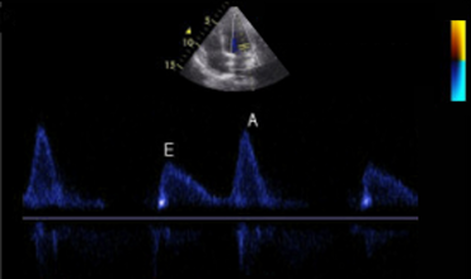 Diastology can often be confusing, as there have many updates to the standards and guidelines regarding how to assess and grade left ventricular diastology in the past few years. So let's dig in to how to assess this and the echocardiographer's role in evaluating diastology based on the updated 2016 ASE Guidelines. So as cardiac sonographers, we should all know the basics... E/A reversal = Diastolic Dysfunction, but there is a little more to it than that. If you're not fully evaluating diastology with additional measures, you're probably missing some positive cases. Also the Intersocietal Accreditation Commission now includes reporting of left ventricular diastolic function as a requirement for echocardiography accreditation. 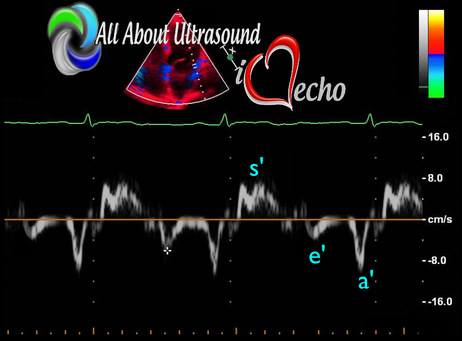 What exactly is diastolic dysfunction? This is a decrease in left ventricular compliance during diastole. While the ejection fraction and left ventricular systolic function are needless to say, pretty important, the diastolic function of the heart is important too. If the heart does not rest properly during diastole, then it cannot fill with the right amount of blood volume needed and eventually this can lead to heart failure and significant clinical implications. So it's important to know the left atrial pressures and end diastolic left ventricular pressures in order to determine the level of severity of the diastolic dysfunction. The updated guidelines break it down like this: Grade 0 = Normal Grade 1 = Impaired Relaxation/Diastolic Dysfunction Grade 2 = Pseudonormalization Grade 3 = Restrictive Pathophysiology So how do we get to the diagnosis? Based on the updated standards from the ASE, determination of normal vs diastolic dysfunction is evaluated initially, based on the patient's EF. If a patient has a normal ejection fraction then the algorithm looks at four components to determine whether or not the patient has a degree of diastolic dysfunction: 1. Average E/e’ > 14 2. e' velocity -Septal e’ velocity < 7 cm/s -Lateral e’ velocity <10 cm/s 3.TR velocity > 2.8 m/s 4. LA volume index >34ml/m2 If <50% are positive, the patient is considered normal. If >50% are positive, the patient has a degree of diastolic dysfunction. If only 50% are positive, then we are unable to determine whether the patient has diastolic dysfunction. If the patient has a compromised ejection fraction, then we can assume that there is a degree of diastolic dysfunction and can grade it based on the E/A ratio. When the mitral inflow pattern shows an E/A ratio <0.8 along with a peak E velocity of <50cm/sec, then the mean LAP is either normal or low and this is considered a Grade 1. When the mitral inflow pattern shows an E/A ratio of >2, the mean LAP is elevated, consistent with Grade 3 diastolic dysfunction. Keep in mind patients with young or athletic patients may show this ratio in the setting of normal diastolic function. Also, patients in atrial fibrillation may exhibit a reduced or loss of the mitral A wave and may also produce similar findings. For patients with reduced EF's that do not meet one of those parameters and the mitral inflow shows an E/A Ratio >0.8 AND the peak E velocity is >50 cm/sec OR E/A Ratio >8 but <2, then other parameters are required for determination of diastolic dysfunction. 1. Average E/e’ Ratio - average E/e’ ratio >14 2. TR Velocity - peak jet velocity >2.8 m/sec 3. LA Volume Index - >34 mL/m2 If 2 of 3 are negative, the patient is considered to have Grade 1 diastolic dysfunction, where if 2 of 3 are positive, then this is considered Grade 2. So, are you confused yet? Let's look at the grading parameters a little closer. GRADE 0 - NORMAL DIASTOLOGYThis means that left atrial pressures (LAP) are normal and the diastolic function is not impaired. The left ventricle relaxes normally throughout diastole and allows for complete diastolic filling. The E/A ratio in a normal setting, is between 1 and 2. This gradually reduces with age and E/A ratio >0.75 may be considered normal above 75 years. 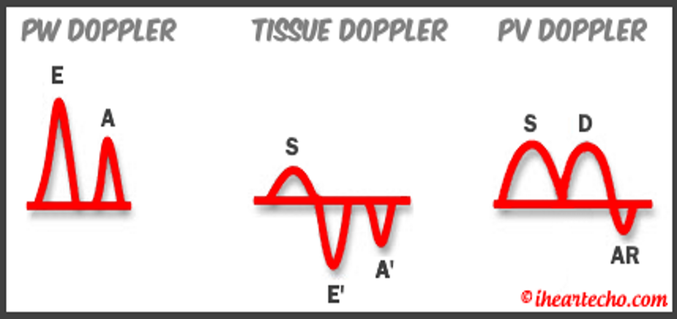 GRADE 1 - IMPAIRED RELAXATION/DIASTOLIC DYSFUNCTIONPatients that do not have a NORMAL EF, will have a degree of diastolic dysfunction and are evaluated based on filling pressures of the left atrium. Left atrial pressures can be somewhat normal in a patient with Grade 1 diastolic dysfunction, but will increased as this progresses. Patients with Grade 1 diastolic dysfunction will have reduced e' velocities and prolonged deceleration time. 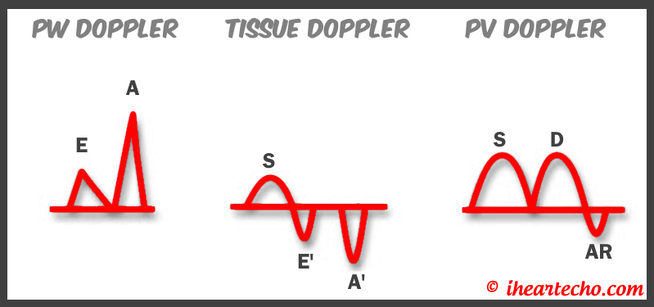 GRADE 2 - PSEUDONORMALIZATIONOne of the biggest factors that our role as sonographers requires, is knowing your patient history. This will often help you know whether or not you're dealing with a normal waveform or pseudonormalization. Granted there are some other key factors but the most obvious is whether or not the patient has previously been diagnosed with diastolic dysfunction. If they have previously had reversal of the E/A waveform and now have a normal waveform pattern, this is a pretty good indicator that the patient is in pseudonormalization. Also, keep in mind some of the other factors associated with increased left atrial pressures, such as blunting or changes to the pulmonary venous waveform, as well as reduced e' velocities. When pseudonormalization is present, the valsalva maneuver can assist to "unload" the ventricle and to reduce filling pressures, causing the E/A reversal to be unmasked. 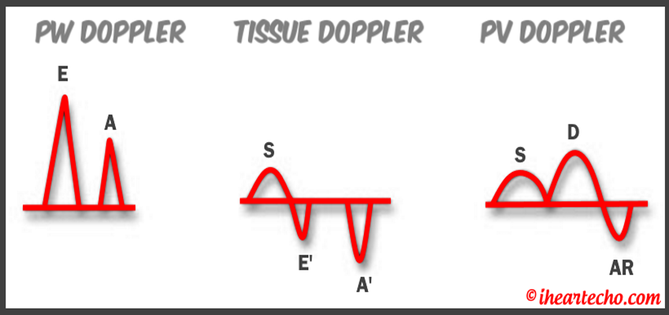 GRADE 3 - RESTRICTIVE FILLING PATTERNGrade 3 diastolic dysfunction involves increased left atrial pressures and increased end diastolic left ventricular pressure. This may result in reversal of the pulmonary venous waveform and is often seen with the presence of left atrial enlargement and left ventricular hypertrophy. 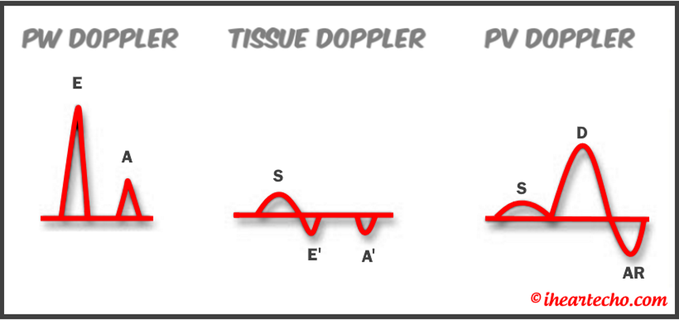 ECHO DIASTOLOGY GRADING ANALYSIS TOOLS!The newly updated algorithm for determining diastology and left atrial pressures can be a little overwhelming and difficult to follow, but we make it easy with our Echocardiography Analysis Tools which include our exclusive LV Diastology Assessment Tool! Quickly and easily determine and grade the diastology based on the updated ASE guidelines. Also there are many other parameters that affect diastology and the application of the diagnostic criteria, such as age, athletic hearts and other factors. Learn and review these additional factors and an in depth study of diastolic dysfunction in our MASTERING LV DIASTOLOGY CME COURSE!
REFERENCE: ASE/EACVI GUIDELINES AND STANDARDS Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging; Nagueh et al
Please note: allaboutultrasound.com and iheartecho.com are not endorsed by or affiliated with the American Society of Echocardiography 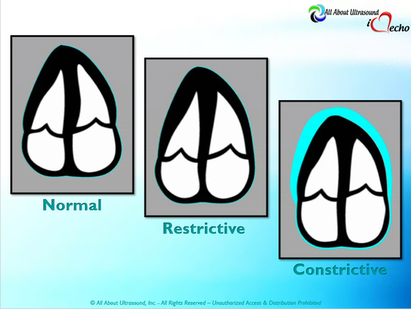 Mastering Echocardiography can be tough, especially when it comes to complex processes like Constrictive Pericarditis. Patients with Constrictive Pericarditis do not present for typical pericarditis symptoms. Instead, they present with symptoms of heart failure and so this can often be a challenge for even very skilled sonographers to identify the subtle differences between Restrictive Cardiomyopathy and Constrictive Pericarditis. These two disease processes can appear very similar on echocardiography. However, there are a few things that clue us into the correct diagnosis. 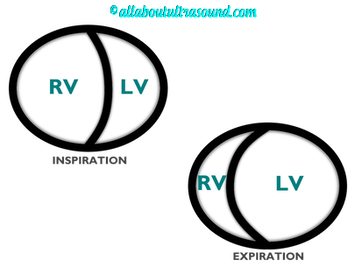 Constrictive Pericarditis is seen with a fibrotic, thickened pericardium, which insulates the ventricle and constricts the ventricle from fully relaxing during diastole. Whereas, Restrictive Cardiomyopathy results in a thickened myocardium, which inhibits the ability of the ventricle to relax and also results in abnormal diastolic function. However, that's where the similarities end. First of all, we need to evaluate for interdependence of the ventricles. But what does that mean? Ventricular interdependence is when there is a respiratory ventricular septal shift. This then leads to an increase in the volume of one ventricle associated with a decreased volume in the opposite ventricle. This can be tricky to diagnose, so it takes a pretty detailed echo exam and a keen eye of the sonographer and physician. 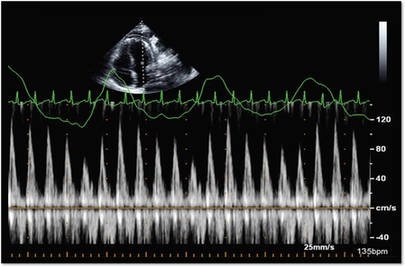 Secondly, when evaluating for constriction, we will need to look at respiratory changes to the Doppler waveform patterns. The respiratory changes in the Mitral inflow pattern will show a variation of greater than 15% when constriction is present. Whereas, with restriction, this waveform pattern will show a restrictive filling pattern with an E/A ratio >2.0 and deceleration time <160ms. 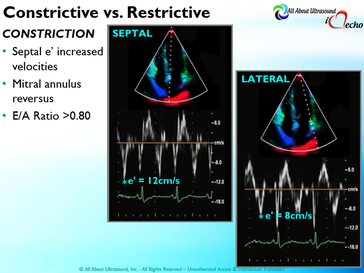 Another key factor in determining constriction vs. restriction is the E/e' ratio and diastolic function. Remember that both disease processes will have a degree of diastolic dysfunction. Normal left ventricular function will typically show a lateral e’ greater than septal/medial e' velocities, because the septal wall is somewhat restricted and the lateral wall is more free to move. However, with constriction the pericardium is insulating the ventricular movements and does not allow for full relaxation and movement of the lateral wall. This results in mitral annulus reversus, which is a decreased lateral e' velocity and compensatory increase in tissue velocities in the septal/medial annulus. Restrictive patterns in tissue velocities will show an overall decrease in both the lateral and septal e' velocities. 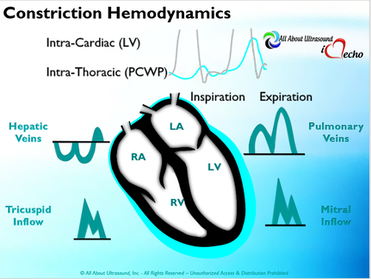 Additionally, with constriction, this will result in expiratory hepatic vein reversal. But why does this occur? Remember that air moves from areas of high pressure to low pressure, which allows for air flow into the lungs. During expiration, the volume of air (and the pressure) of the thoracic cavity decreases, causing the intrapulmonary pressure to rise above the atmospheric pressure. However, with constriction, the pericardium is insulating the intracardiac chambers and this keeps them from tracking normally with intrapulmonary pressures. Remember the pulmonary artery and aorta are OUTSIDE of the pericardium. So with constriction the thorax pressure and the pulmonary venous pressure will drop, but there are phasic filling differences within the heart, because the gradient to fill the left side of the heart is decreased. The heart is no longer able to push outward against the pericardium, so the pressure is forced inward into the cardiac chambers. So during expiration, the pressure in the right atrium causes flow reversal in the hepatic veins. Whereas, with chronic late stages of restriction, there is an inspiratory reversal during diastole, because there is no shifting of septum and the right heart cannot accommodate increased flow which results from chronic diastolic dysfunction and this causes hepatic vein reversal. While diagnosing Constrictive Pericarditis on echocardiography can certainly be a challenge, it can be done with confidence. Paying close attention to the details and recognizing when your patient with heart failure symptoms might actually be more than meets the eye, can help to make the correct diagnosis and ensure adequate treatment for your patient. Want more information on the differences between Constrictive Pericarditis and Restrictive Cardiomyopathy, including Strain Imaging methods? See our E-Learning Course Mastering Constrictive Pericarditis and earn 1 SDMS CME credit. REFERENCES
Scanning Tip: Q: What's a great way to help delineate the pancreas on an abdominal ultrasound? A: Have the patient drink water at the end of the exam and re-image the pancreas. This will help delineate the pancreas. Also sitting the patient in an erect position can assist with imaging the pancreas. Scan On! www.allaboutultrasound.com 
|

Making Waves™All About Ultrasound presents Making Waves™, our ultrasound specific blog and newsletter. Join us here for ultrasound news, cases and more! Don't FORGET YOUR MERCH!
Archives
May 2023
Categories
All
|


 RSS Feed
RSS Feed