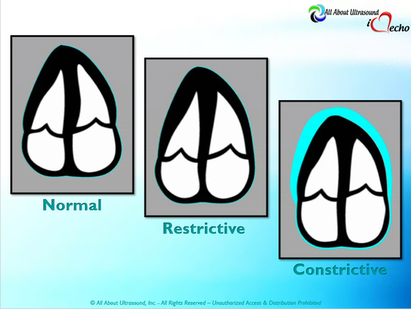
 Mastering Echocardiography can be tough, especially when it comes to complex processes like Constrictive Pericarditis. Patients with Constrictive Pericarditis do not present for typical pericarditis symptoms. Instead, they present with symptoms of heart failure and so this can often be a challenge for even very skilled sonographers to identify the subtle differences between Restrictive Cardiomyopathy and Constrictive Pericarditis. These two disease processes can appear very similar on echocardiography. However, there are a few things that clue us into the correct diagnosis. 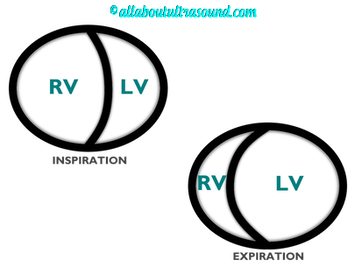 Constrictive Pericarditis is seen with a fibrotic, thickened pericardium, which insulates the ventricle and constricts the ventricle from fully relaxing during diastole. Whereas, Restrictive Cardiomyopathy results in a thickened myocardium, which inhibits the ability of the ventricle to relax and also results in abnormal diastolic function. However, that's where the similarities end. First of all, we need to evaluate for interdependence of the ventricles. But what does that mean? Ventricular interdependence is when there is a respiratory ventricular septal shift. This then leads to an increase in the volume of one ventricle associated with a decreased volume in the opposite ventricle. This can be tricky to diagnose, so it takes a pretty detailed echo exam and a keen eye of the sonographer and physician. 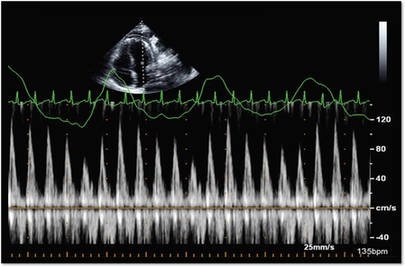 Secondly, when evaluating for constriction, we will need to look at respiratory changes to the Doppler waveform patterns. The respiratory changes in the Mitral inflow pattern will show a variation of greater than 15% when constriction is present. Whereas, with restriction, this waveform pattern will show a restrictive filling pattern with an E/A ratio >2.0 and deceleration time <160ms. 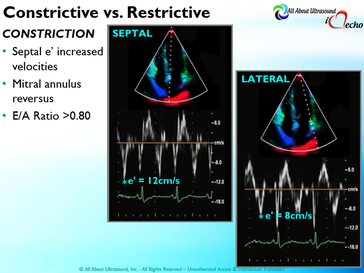 Another key factor in determining constriction vs. restriction is the E/e' ratio and diastolic function. Remember that both disease processes will have a degree of diastolic dysfunction. Normal left ventricular function will typically show a lateral e’ greater than septal/medial e' velocities, because the septal wall is somewhat restricted and the lateral wall is more free to move. However, with constriction the pericardium is insulating the ventricular movements and does not allow for full relaxation and movement of the lateral wall. This results in mitral annulus reversus, which is a decreased lateral e' velocity and compensatory increase in tissue velocities in the septal/medial annulus. Restrictive patterns in tissue velocities will show an overall decrease in both the lateral and septal e' velocities. 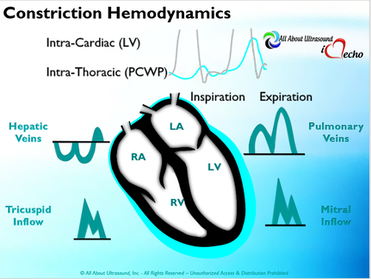 Additionally, with constriction, this will result in expiratory hepatic vein reversal. But why does this occur? Remember that air moves from areas of high pressure to low pressure, which allows for air flow into the lungs. During expiration, the volume of air (and the pressure) of the thoracic cavity decreases, causing the intrapulmonary pressure to rise above the atmospheric pressure. However, with constriction, the pericardium is insulating the intracardiac chambers and this keeps them from tracking normally with intrapulmonary pressures. Remember the pulmonary artery and aorta are OUTSIDE of the pericardium. So with constriction the thorax pressure and the pulmonary venous pressure will drop, but there are phasic filling differences within the heart, because the gradient to fill the left side of the heart is decreased. The heart is no longer able to push outward against the pericardium, so the pressure is forced inward into the cardiac chambers. So during expiration, the pressure in the right atrium causes flow reversal in the hepatic veins. Whereas, with chronic late stages of restriction, there is an inspiratory reversal during diastole, because there is no shifting of septum and the right heart cannot accommodate increased flow which results from chronic diastolic dysfunction and this causes hepatic vein reversal. While diagnosing Constrictive Pericarditis on echocardiography can certainly be a challenge, it can be done with confidence. Paying close attention to the details and recognizing when your patient with heart failure symptoms might actually be more than meets the eye, can help to make the correct diagnosis and ensure adequate treatment for your patient. Want more information on the differences between Constrictive Pericarditis and Restrictive Cardiomyopathy, including Strain Imaging methods? See our E-Learning Course Mastering Constrictive Pericarditis and earn 1 SDMS CME credit. REFERENCES
2 Comments
|

Making Waves™All About Ultrasound presents Making Waves™, our ultrasound specific blog and newsletter. Join us here for ultrasound news, cases and more! Don't FORGET YOUR MERCH!
Archives
May 2023
Categories
All
|
 RSS Feed
RSS Feed